What is HCC?
Hepatocellular carcinoma (HCC) is the most common primary liver cancer. It arises predominantly in patients with chronic liver disease or cirrhosis - a population that undergoes routine surveillance imaging. Critically, HCC is one of the few cancers where imaging alone can establish a diagnosis; no biopsy is required. This is codified in the LI-RADS framework.
What is LI-RADS?
LI-RADS (Liver Imaging Reporting and Data System) standardizes the description and categorization of liver observations on contrast-enhanced CT and MRI in patients at high risk for HCC. It assigns each observation a category based on imaging features.
The LI-RADS framework follows a strict clinical logic built on temporal analysis. Multiple contrast phases are acquired: before contrast injection (non-contrast) and at successive time points after injection (arterial, portal venous, and delayed) to capture how the lesion's enhancement changes over time relative to the surrounding liver.
Please refer to the official Liver Imaging Reporting and Data System (LI-RADS)® definition.
Category overview
| Category | Meaning |
|---|---|
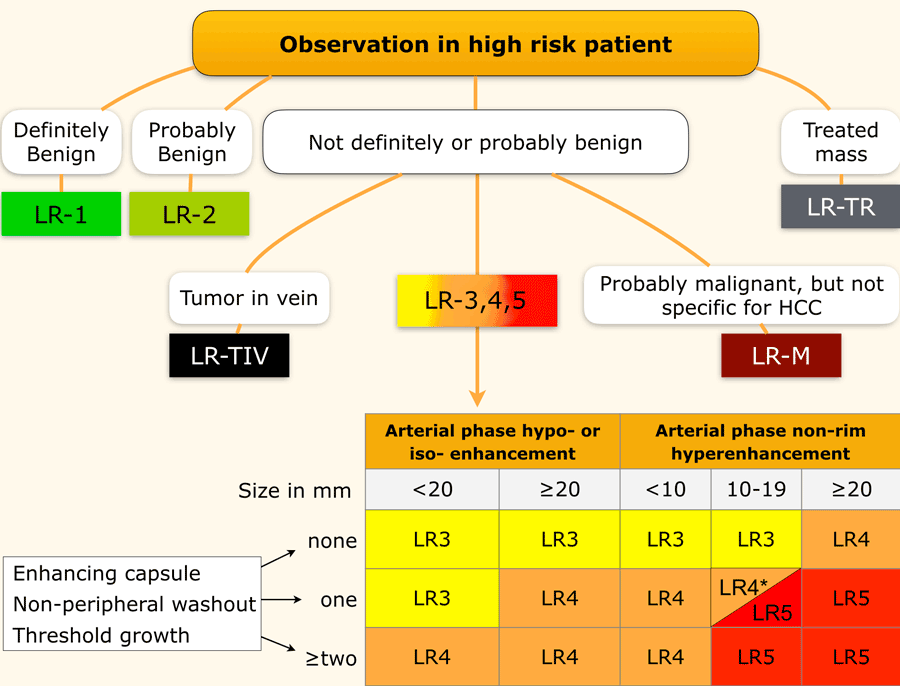
| LR-1 | Definitely benign |
| LR-2 | Probably benign |
| LR-3 | Intermediate probability for HCC |
| LR-4 | Probably HCC |
| LR-5 | Definitely HCC |
| LR-M | Probably malignant, not HCC-specific |
| LR-TIV | Tumor in vein |
Major imaging features
LI-RADS defines specific enhancement features that, when present, raise concern for HCC. Four major features are evaluated:
- Arterial phase hyperenhancement (APHE) - the lesion enhances brighter than the surrounding liver in the early arterial phase, reflecting the abnormal arterial supply that characterizes HCC. Only non-rim APHE counts - enhancement limited to the outer edge of the lesion (rim pattern) suggests a different diagnosis.
- Non-peripheral washout - in the portal venous or delayed phase, the lesion becomes relatively darker than the surrounding liver. This reflects contrast washing out of the tumor faster than the background liver parenchyma.
- Enhancing capsule - a thin bright rim persisting at the lesion edge in the portal venous or delayed phase. This reflects contrast being retained in the fibrous tissue that surrounds and encases the tumor.
- Threshold growth - a significant increase in lesion size over a short interval (≥50% diameter growth in ≤6 months), reflecting rapid tumor proliferation (not present as a label in the challenge dataset).
Confirming HCC from imaging requires placing a lesion into the LR-3, LR-4, or LR-5 range - which reflects increasing probability of HCC from intermediate to definite. The algorithm for reaching those categories is built on the features above.
How are LR-3 through LR-5 determined?
The primary gating feature is non-rim APHE. Lesions without non-rim APHE can reach a maximum of LR-4, regardless of size or other features. Lesions with non-rim APHE are then categorized by a combination of size and how many additional major features are present (washout, capsule, or threshold growth) - more features and larger size push the category higher, from LR-3 up to LR-5.